The simplicity of one partner with the resources of many.
The Affordable Care Act created exciting new opportunities to achieve the ‘Triple Aim’ of improving care, improving health, and lowering costs, by creating a comprehensive, coordinated, patient-centered system of care. And now, the realization that social determinants of health can have greater impact on health than medical care, is leading to innovative partnerships between health care systems and social service agencies. These partnerships help meet the needs of high-risk/high-cost populations and achieve better health at a lower cost.
Partners at Home (PAH) is a specialty network of Community-Based Organizations (CBOs) leading the nation in prototyping models to provide patient-centered social services in the home and community. We offer a statewide network of providers supporting a variety of specialty services, including social care management, disease self-management and wellness, personal care, homemaker and respite services (private duty), loneliness and social isolation interventions, and meals.
Led by Partners in Care Foundation, a CBO accredited for Complex Case Management by the National Committee for Quality Assurance (NCQA), the PAH Network addresses vital drivers of health outcomes, including issues responsible for preventable emergency department use, hospitalizations, and nursing home admissions.

Why Collaborate with the Partners at Home Network?
The Partners at Home Network streamlines access to multiple community-based care “extenders,” providing hospitals, physician groups and health plans with a simple, efficient, “one call does it all” coordinated community care system, staffed with a well-trained, culturally and linguistically competent workforce, experienced in helping patients whose health is fragile, and their care complex and costly.
Our Array of Services
The Partners at Home Network addresses the social determinants of health, including issues related to preventable ED use, hospitalizations, and nursing home admissions. We do this in two ways:
1. Short-Term Service Coordination & Long-Term Services and Supports – the provision of services including: home medication review (HomeMeds), Care Transitions, behavioral health interventions, and wraparound support services encompassing in-home assessments, medication management, safety evaluations, home-delivered meals, medical transportation and more.
In summary:
- A single point of access to a large spectrum of services, scalable for regional and state coverage
- Coordination of resources (medication management, home services, meal delivery, etc.) provided at a competitive price
- Continuity of services provided by culturally different providers with local expertise to engage patients in their own outcomes
- Quality-accredited provider of a full-continuum of patient centered services
2. Health Self-Management Education – In a groundbreaking departure from traditional approaches to chronic disease management, Partners created a contact center to pilot a unique outreach program, specifically designed to boost engagement in health self-management education.
The contact details of thousands of pre-screened health plan members are mapped to identify aggregations of sufficient numbers to form a workshop. Members within convenient driving distance of a workshop are then called, and those who indicate potential interest are connected to agents trained to assist the member in identifying which modality of self-management workshop best fits their lifestyle.
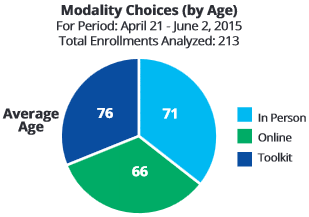
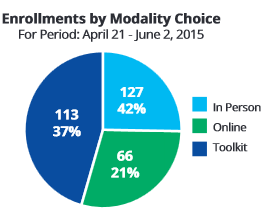
Participants are offered one of three programs developed by Stanford University School of Medicine:
- Six, 2.5 hour in-person workshops
- An online program of health self-management activities
- A toolkit, containing a workbook to aid the development of skills to self-manage chronic conditions, and a relaxation and exercise CD
Our Results
The Partners at Home Network has achieved significant results.
1. Short-Term Service Coordination & Long-Term Services and Supports
- Our Care Transitions coaches providing social service coordination in Glendale, cut 30-day readmissions to the three hospitals served in the Glendale collaborative from 21.6% in first quarter the collaborative started CCTP intervention (May-July 2013), to 12.1% in the most recent quarter for which data exists (Aug-Oct 2014.)
- Providing Long-Term Services and Supports for the dually eligible for Medicare and MediCal population kept nursing-home eligible seniors at home for an average of five years at a cost of $357/month versus $3,000+/month skilled nursing facility cost.
- A study conducted by a leading physician group on our HomeMeds medication management interventions revealed that adults who received a home care visit, had their medications reviewed by a consulting pharmacist and received a psychological/functional needs assessment and home safety evaluation had a 13% lower rate of emergency department use and 22% fewer readmissions within 30 days when compared to those who received no intervention.
- Pharmacists who conducted a medication evaluation as part of the HomeMeds program recommended medication changes in 63% of the cases reviewed.
2. Health Self-Management Education
Early results of the contact center outreach pilot are extremely promising. The pilot has seen an initial outreach to approximately 8,000 individuals with chronic conditions in Los Angeles County. Approximately 10% of those contacted expressed interest in participating in the program and 36% of individuals who expressed interest enrolled in one of the three modalities mentioned above. The illustrations below show program sign up by modality and median age.
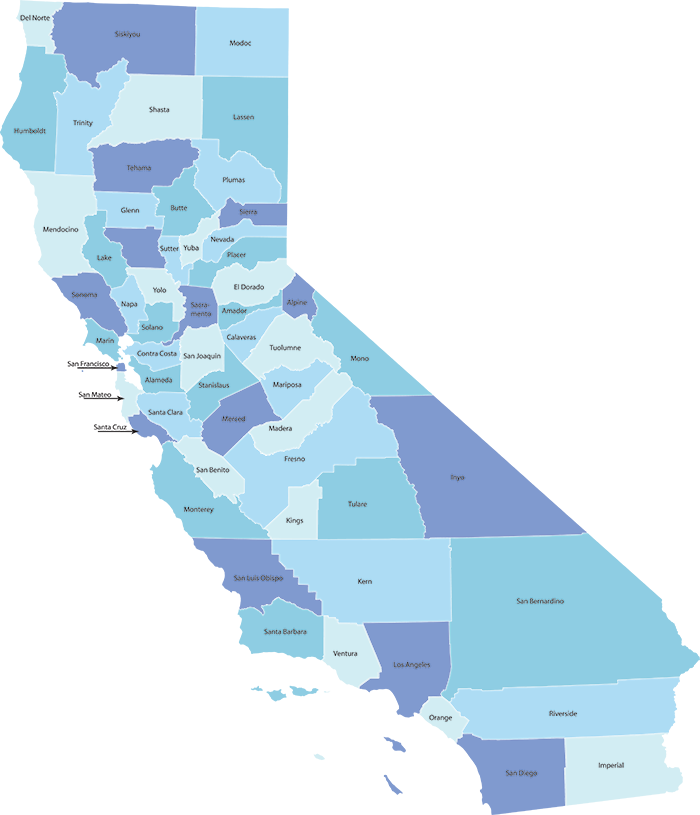
Where Do We Provide Services?
The Partners at Home Network provides services in communities and counties across California.